Coil Embolization of a Left Circumflex Feeder Branch in a Patient With a Mediastinal Paraganglioma
Images in Intervention
Introduction
A 62-year-old man presented with several months of fatigue, palpitations, and dyspnea on exertion. A Holter monitor revealed a high burden of multifocal premature ventricular contractions (>110/h) with a 9-beat run of nonsustained ventricular tachycardia. Transthoracic echocardiogram showed normal resting left ventricular systolic function with no valvular abnormalities. On a stress echocardiogram, the patient achieved 12 METs, 85% of maximum predicted heart rate, with no ischemic electrocardiogram findings or stress-induced wall motion abnormalities. He had a short run of supraventricular tachycardia during stress that spontaneously resolved. Due to progression of his dyspnea, he was referred for coronary angiography, which revealed no angiographic evidence of coronary artery disease. However, a large tortuous vessel, originating from the proximal left circumflex artery, was visualized coursing superiorly toward an enhancing extracardiac mass lesion (Fig. 1A). Contrast-enhanced computed tomography of the thorax revealed a 2.8 × 2.3 × 3.6 cm, heterogeneous, hypervascular mass adjacent to the left atrium and abutting the left superior pulmonary vein (Fig. 1B). A positron emission tomography scan showed the mass to be intensely radiotracer-avid with a standard uptake value maximum of 21.3 (Fig. 1C). The treatment strategy was to gain hemostatic control before surgical resection. The patient underwent percutaneous coronary coil embolization of the tumor feeder branch with transcatheter placement of 9 platinum detachable coils (MicroPlex Coil System, Terumo Medical, Somerset, New Jersey) with dramatic reduction in distal blood flow (Fig. 2A). The patient then underwent surgical resection via a left thoracotomy. The pericardium was incised, revealing the mass adjacent to the left inferior pulmonary vein at its junction with the left atrium (Fig. 2B). Anatomic left lower lobectomy was performed with en bloc resection of the mass. Of note, intraoperative manipulation of the mass resulted in severe hypertension, suggesting a functional tumor. Pathology revealed a paraganglioma with negative margins.

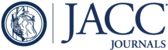
Coronary Angiogram, CT, and PET
(A) Initial coronary angiogram: coronary angiography showing a large tortuous vessel originating from the proximal left circumflex supplying a hypervascular mass. (B) Cardiac computed tomography (CT): maximum intensity projection image showing mass adjacent to the left atrium (LA) and the left pulmonary vein. (C) Fluoro-18-deoxyglucose positron emission tomography (PET) imaging scan showing high radiotracer uptake in the mediastinal mass. Ao = aorta; PA = pulmonary artery.

Coronary Angiography and Intraoperative Photograph
(A) Intracoronary coil implantation: coronary angiography after implantation of coils in the tumor feeder vessel. (B) Intrapericardial mass: intraoperative photograph demonstrating an intrapericardial mass involving left inferior pulmonary vein.
Footnotes
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
{kind=link}
{kind=link}