Long-Term Safety and Effectiveness of Drug-Eluting Stents for the Treatment of Saphenous Vein Grafts Disease: A Population-Based Study
Clinical Research
Objectives:
The purpose of this study was to evaluate the long-term safety and effectiveness of drug-eluting stents (DES) for the treatment of saphenous vein graft (SVG) disease.
Background:
DES are frequently implanted for SVG interventions, but some studies have shown that they are not effective in reducing target vessel revascularization (TVR) over longer-term follow-up. Some studies suggest there is increased mortality with DES compared with bare-metal stents (BMS).
Methods:
We performed propensity score matching analysis using a population-based cohort that included 709 well-matched pairs (n = 1,418) who received DES or BMS for the treatment of SVG disease from 2003 to 2008. Outcomes of interest included repeat TVR, myocardial infarction, and death.
Results:
The mean age of the propensity-matched cohort was 69 years, 50% had diabetes, and the mean age of SVG was 10.6 years. At 4-year follow-up, the rate of repeat TVR was 21% in the DES group and 27.6% in the BMS group (p = 0.004). DES implantation was associated with the largest TVR reduction among patients with diabetes and patients receiving longer stents (≥30 mm) and the number of procedures needed to prevent a TVR at 4 years was 8 and 7, respectively. The composite rate of myocardial infarction or death was not significantly different between DES and BMS at 4 years (27.8% vs. 32.6%, p = 0.09).
Conclusions:
Implantation of DES in the treatment of SVG disease is associated with substantial reduction of repeat revascularization, without evidence of an increased risk of myocardial infarction or death at longer-term follow-up.
Introduction
Drug-eluting stents (DES) have been demonstrated to be safe and highly effective in reducing the need for repeat coronary revascularization in native coronary vessels and have been adopted to the routine practice of interventional cardiology (1–3). Although it is hoped that the benefits of DES can be extended to the treatment of saphenous vein graft (SVG) lesions, there are existing concerns and controversies regarding the safety and effectiveness of DES in the treatment of SVG disease (4,5). In the RRISC (Reduction of Restenosis in Saphenous Vein Grafts with Cypher Stent) trial (6,7), substantially higher rates of death were seen among patients treated with DES compared with bare-metal stents (BMS) (29% in the DES group vs. 0% in the BMS group) during a median follow-up of 32 months. The recently published long-term follow-up of the SOS (Stenting of Saphenous Vein Grafts) trial (8) also showed increased in all-cause mortality associated with DES (24% in the DES group vs. 13% in the BMS group) that did not reach statistical significance. Although several observational studies (9–11) and meta-analyses (12–14) have reported no increased risks of death or recurrent myocardial infarction associated with DES implantation in SVG disease, limitations of these studies have even led study investigators to urge cautious interpretation of their findings.
In the 25 studies (3 randomized, 22 observational) that assessed DES for the treatment of SVG disease, only 7 studies assessed longer-term outcomes of more than 30 months (13). All 7 studies were single-center cohorts, which raised concerns regarding the generalizability of the findings. Only 1 of 25 studies evaluated more than 500 patients in the DES group (13). Although meta-analyses can increase the accuracy of estimates, this statistical technique cannot eliminate selection biases inherent to these small observational studies (15). Finally, several studies have suggested a “catch up” phenomenon whereby the early benefits of DES in reducing repeat revascularization are attenuated over time, and that DES are no longer more effective than BMS at longer term (7,9,16). Yet, very few studies have adjusted for the potential difference in the degree of degeneration in SVGs, thus potentially biasing against the DES group at longer-term because they are often implanted among patients with higher risk of disease progression.
In the United States, it is estimated that SVG interventions account for 5% to 10% of the total number of percutaneous coronary interventions (PCI) performed each year (12). Addressing these gaps in knowledge may have a significant impact on the practice of interventional cardiology. The availability of a large population-based PCI database in Ontario, Canada, afforded a unique opportunity to conduct 1 of the largest and most comprehensive studies to evaluate the long-term safety and effectiveness of DES versus BMS in patients undergoing SVG interventions.
Methods
Data sources
Data sources
The Cardiac Care Network (CCN) of Ontario maintains an ongoing prospective clinical registry of all patients undergoing cardiac catheterization, PCI, and coronary artery bypass graft (CABG) surgery (17,18). Since the introduction of DES in late 2003, specific mandatory fields such as stent type, size and diameter of each stent, and location of stent placement were added. The Canadian Institute for Health Information hospital discharge abstract database was used to identify additional comorbid conditions not captured in the CCN registry and to identify repeat hospitalization after the index PCI procedure. The Ontario Registered Persons Database was used to ascertain mortality outcomes. Linkages of these large databases were performed using unique encrypted patient identifiers to protect patient confidentiality. The need for informed patient consent was waived because participation is mandatory under Ontario's legislation regarding the privacy of health information. This study was approved by the research ethics board at the Sunnybrook Health Sciences Centre.
Study sample
We identified an initial cohort of patients who underwent stent implantation for the treatment of SVG disease from December 1, 2003, to December 31, 2008. This time frame was chosen to allow for at least 1 year of follow-up for each patient. From this initial cohort, we excluded patients who had both DES and BMS during the index PCI. We also excluded patients who had PCI or CABG in the 12 months before the index procedure using data from the CCN registry because of the concern that there would not be a sufficient number of patients receiving BMS to allow for propensity score matching. Patients who did not have a valid Ontario health card number were also excluded because their outcomes could not be determined.
Outcomes
The primary effectiveness outcome was repeat target vessel revascularization (TVR). The primary safety outcomes were myocardial infarction and all-cause mortality. Repeat TVR after the index PCI was determined using information from the CCN database. Recurrent myocardial infarction leading to hospitalization was assessed using the Canadian Institute for Health Information discharge abstract database (International Classification of Diseases- 10th revision, disease codes I21 and I22). Periprocedure myocardial infarctions after PCI were not included in outcome assessment. Mortality was determined from the Ontario Registered Persons Database. Complete follow-up data were available for each patient through March 31, 2010, for all outcomes of interest.
Statistical analysis
Propensity score matching analysis was used to minimize the influence of potential confounding and selection biases (17–20). We calculated the predicted probability of DES implantation by fitting a logistic regression model using all the clinically relevant variables for stent selection from clinical knowledge. As shown in Table 1, these variables included demographics (age, sex), comorbidities (hypertension, diabetes, cerebrovascular disease, chronic obstructive pulmonary disease, heart failure, peripheral vascular disease, cancer, hemodialysis), admission characteristics (angina classification, myocardial infarction), and procedure characteristics (stent location, stent size, stent length). We also adjusted for the age of SVGs by calculating the time of CABG to index PCI as a surrogate for the degree of SVG degeneration. A greedy, nearest-neighbor 1:1 matching algorithm was used to match patients, with matching occurring if the difference in the logits of the propensity scores was <0.2× the SD of the scores (caliper width) (19,20). Patients were used only in 1 propensity score matched pair, and those without a suitable match were excluded from the analysis. After constructing a propensity-matched cohort, we assessed the degree of balance in measured covariates between the DES group and the BMS group. We computed the standardized difference between the 2 groups for each type of distribution, with differences of less than 0.1 taken to indicate good balance in the matched cohort. Kaplan-Meier survival curves between the DES group and the BMS group were compared using appropriate statistical tests for matched data (19,20).
| Total (N = 1,418) | BMS (n = 709) | DES (n = 709) | |
|---|---|---|---|
| Demographics | |||
| Age, yrs | 69.5±9.2 | 69.7±9.3 | 69.2±9.0 |
| <65 | 399(28.1%) | 195(27.5%) | 204(28.8%) |
| 65–74 | 575(40.6%) | 286(40.3%) | 289(40.8%) |
| 75–84 | 403(28.4%) | 207(29.2%) | 196(27.6%) |
| ≥85 | 41(2.9%) | 21(3.0%) | 20(2.8%) |
| Male | 1,178(83.1%) | 584(82.4%) | 594(83.8%) |
| Admission characteristics | |||
| Recent AMI (same day as PCI) | 98(6.9%) | 54(7.6%) | 44(6.2%) |
| Recent AMI (days 1–7) | 249(17.6%) | 126(17.8%) | 123(17.3%) |
| Recent AMI (days 8–30) | 89(6.3%) | 39(5.5%) | 50(7.1%) |
| No prior AMI within 30 days before PCI | 982(69.3%) | 490(69.1%) | 492(69.4%) |
| CCS angina class before procedure | |||
| 0 | 48(3.4%) | 23(3.2%) | 25(3.5%) |
| I | 38(2.7%) | 18(2.5%) | 20(2.8%) |
| II | 182(12.8%) | 86(12.1%) | 96(13.5%) |
| III | 358(25.2%) | 184(26.0%) | 174(24.5%) |
| IV | 750(52.9%) | 377(53.2%) | 373(52.6%) |
| Time from CABG to index PCI, yrs | 10.6±4.3 | 10.6±4.2 | 10.6±4.3 |
| 1–5 | 131(9.2%) | 66(9.3%) | 65(9.2%) |
| 5–10 | 320(22.6%) | 159(22.4%) | 161(22.7%) |
| >10 | 660(46.5%) | 333(47.0%) | 327(46.1%) |
| Missing | 307(21.7%) | 151(21.3%) | 156(22.0%) |
| Cardiac risk factors and comorbidities | |||
| Hypertension | 889(62.7%) | 451(63.6%) | 438(61.8%) |
| Diabetes | 714(50.4%) | 353(49.8%) | 361(50.9%) |
| Prior stroke or transient ischemic attack | 84(5.9%) | 43(6.1%) | 41(5.8%) |
| Chronic obstructive pulmonary disease | 93(6.6%) | 44(6.2%) | 49(6.9%) |
| Heart failure | 204(14.4%) | 104(14.7%) | 100(14.1%) |
| Peripheral vascular disease | 245(17.3%) | 126(17.8%) | 119(16.8%) |
| Cancer | 14(1.0%) | 7(1.0%) | 7(1.0%) |
| Hemodialysis | 21(1.5%) | 10(1.4%) | 11(1.6%) |
| Stent location | |||
| SVG to left anterior descending or diagonal | 368(26.0%) | 193(27.2%) | 175(24.7%) |
| SVG to left circumflex | 574(40.5%) | 280(39.5%) | 294(41.5%) |
| SVG to right coronary artery | 543(38.3%) | 269(37.9%) | 274(38.6%) |
| Stent characteristics | |||
| Number of stents | 1.59±0.90 | 1.56±0.85 | 1.61±0.96 |
| Stent diameter | 3.15±0.51 | 3.15±0.52 | 3.15±0.51 |
| Stent length | 18.4±5.8 | 18.2±5.9 | 18.5±5.7 |
In pre-specified subgroup analyses of the outcome TVR, patients in the DES group and those in the BMS group were matched on the basis of stent length (long [≥30 mm] vs. short [<30 mm]), stent diameter (small [<3 mm] vs. large [≥3 mm]), diabetes status (presence vs. absence), time from CABG to index PCI (<10 years vs. ≥10 years), and the logit of the propensity score. Within each of the subgroups, the reduction in the risk of the outcome was compared between the DES group and the BMS group using a Cox regression model, with stent type as the sole predictor variable. Robust standard errors that accounted for the clustering of pairs in the matched cohort were obtained (19,20). The number of patients who would need to be treated to prevent 1 repeat TVR event was also calculated.
SAS (version 9.1, SAS Institute, Cary, North Carolina) was used for statistical analyses. A 2-sided p value of 0.05 or less was considered as statistically significant in the comparison of outcomes.
Results
Study sample
Study sample
From December 1, 2003, to December 31, 2008, 81,871 patients underwent PCI procedures in Ontario, Canada, and 2,961 patients received stent implantation for SVG disease. After excluding 263 patients who had both DES and BMS, 398 patients who had PCI or CABG within 12 months of the index procedure, and considered the initial PCI among those with multiple procedures during the study period, our final study cohort included 2,222 patients. Among them, 803 patients received DES and 1,419 patients received BMS. The baseline characteristics in the DES group and the BMS group before propensity score matching are shown in Online Table 1.
Baseline characteristic in the propensity-matched cohort
We identified 709 matched pairs (N = 1,418) who had similar likelihood of receiving DES or BMS after propensity score matching. The mean age was 69 years, 83% were men, and 50% had a history of diabetes (Table 1). The mean duration from CABG to the index PCI was 10.6 years. The majority (65.6%) of patients in the DES group received paclitaxel-eluting stents. The median follow-up was 42 months in the DES group and 39 months in the BMS group. All the demographics, clinical, and procedural characteristics were well balanced between the matched pairs of DES and BMS patients. None of the admission or procedure characteristics had a standardized difference of the means exceeding 0.1 (Table 1).
Target vessel revascularization
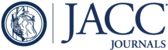
Overall, 21% of the patients receiving a DES and 27.6% of those receiving a BMS required repeat TVR by 4 years (p = 0.004) (Table 2,Fig. 1). The reduction in repeat TVR associated with DES was observed at 6 months and remained significantly lower than BMS throughout the study period. However, the effectiveness of DES on reducing TVR varied substantially according to the pre-specified subgroups (Table 3). For example, the number of procedures needed to prevent TVR at 4 years was 8 for patients with diabetes and 7 for patients with stent length ≥30 mm. In contrast, the number needed to treat was 228 for nondiabetic patients and 51 for patients with shorter stent length <30 mm (Table 3).
| Outcomes⁎ | BMS (n = 709) | DES (n = 709) | p Value† |
|---|---|---|---|
| Target vessel revascularization, % | 0.004 | ||
| 6 months | 7.8 | 4.3 | |
| 1 yr | 12.5 | 8.0 | |
| 1.5 yrs | 16.1 | 10.6 | |
| 2 yrs | 18.6 | 12.9 | |
| 2.5 yrs | 21.7 | 15.6 | |
| 3 yrs | 23.6 | 16.9 | |
| 3.5 yrs | 25.6 | 19.5 | |
| 4 yrs | 27.6 | 21.0 | |
| Myocardial infarction, % | 0.56 | ||
| 6 months | 3.4 | 2.7 | |
| 1 yr | 6.7 | 5.1 | |
| 1.5 yrs | 9.0 | 6.9 | |
| 2 yrs | 10.2 | 7.9 | |
| 2.5 yrs | 11.8 | 9.8 | |
| 3 yrs | 14.1 | 11.7 | |
| 3.5 yrs | 16.4 | 13.0 | |
| 4 yrs | 18.4 | 15.0 | |
| Death, % | 0.17 | ||
| 6 months | 6.2 | 3.1 | |
| 1 yr | 8.5 | 5.6 | |
| 1.5 yrs | 11.6 | 7.4 | |
| 2 yrs | 14.2 | 10.3 | |
| 2.5 yrs | 15.8 | 11.6 | |
| 3 yrs | 17.2 | 14.1 | |
| 3.5 yrs | 18.2 | 16.1 | |
| 4 yrs | 21.1 | 18.5 | |
| Myocardial infarction or death, % | 0.09 | ||
| 6 months | 8.7 | 5.4 | |
| 1 yr | 13.5 | 9.4 | |
| 1.5 yrs | 18.0 | 12.6 | |
| 2 yrs | 21.1 | 16.2 | |
| 2.5 yrs | 23.7 | 18.9 | |
| 3 yrs | 26.4 | 22.0 | |
| 3.5 yrs | 29.1 | 24.8 | |
| 4 yrs | 32.6 | 27.8 |

TVR Comparing DES and BMS
Kaplan-Meier cumulative event curves for target vessel revascularization (TVR) in the propensity-matched cohort showing significant reduction in TVR rates in the drug-eluting stent (DES) group. Light blue line = DES; dark blue line = bare-metal stents (BMS). The p value was estimated using log-rank test for paired sample. PCI = percutaneous coronary intervention.
| Characteristics | Matched Pairs (n) | BMS (%) | DES (%) | HR (95% CI)† | p Value | NNT |
|---|---|---|---|---|---|---|
| Diabetes | ||||||
| Yes | 366 | 32.4 | 19.3 | 0.61(0.42–0.89) | 0.01 | 8 |
| No | 343 | 21.8 | 21.3 | 0.67(0.44–1.02) | 0.06 | 228 |
| Stent size, mm | ||||||
| ≥3.0 | 490 | 28.3 | 22.1 | 0.68(0.49–0.95) | 0.02 | 16 |
| <3.0 | 216 | 23.3 | 19.9 | 0.61(0.35–1.09) | 0.09 | 29 |
| Stent length, mm | ||||||
| ≥30 | 244 | 34.1 | 19.3 | 0.59(0.38–0.91) | 0.02 | 7 |
| <30 | 465 | 24.0 | 22.0 | 0.90(0.63–1.27) | 0.54 | 51 |
| Time from CABG to index PCI, yrs | ||||||
| ≥10 | 338 | 30.0 | 23.4 | 0.73(0.50–1.07) | 0.10 | 15 |
| <10 | 221 | 26.3 | 20.9 | 0.65(0.40–1.07) | 0.09 | 19 |
Myocardial infarction and death
The rate of myocardial infarction during the study period did not differ significantly between the DES and the BMS groups (p = 0.56) (Table 2, Fig. 2). At 4 years, the rate of death was 18.5% in the DES group and 21.1% in the BMS group, which is also not significantly different (p = 0.17) (Table 2, Fig. 3). The composite endpoint of myocardial infarction or death at 4 years occurred in 27.8% in the DES group as compared to 32.6% in the BMS group, but this difference did not reach statistical significance (p = 0.09) (Table 2, Fig. 4).

MI Comparing DES and BMS
Kaplan-Meier cumulative event curves for myocardial infarction (MI) in the propensity-matched cohort showing no significant increase in MI rates associated with DES. Light blue line = DES; dark blue line = BMS. The p value was estimated using log-rank test for paired sample. Abbreviations as in Figure 1.

Death Comparing DES and BMS
Kaplan-Meier cumulative event curves for MI in the propensity-matched cohort showing no significant increase in mortality rates associated with DES. Light blue line = DES; dark blue line = BMS. The p value was estimated using log-rank test for paired sample. Abbreviations as in Figures 1 and 2.

MI or Death Comparing DES and BMS
Kaplan-Meier cumulative event curves for MI in the propensity-matched cohort showing no significant increase in MI or death rates associated with DES. Light blue line = DES; dark blue line = BMS. The p value was estimated using the log-rank test for paired sample. Abbreviations as in Figures 1 and 2.
Discussion
Our study extends previous findings by conducting the largest observational study to-date evaluating the long-term safety and effectiveness of DES for the treatment of SVG disease. First, we did not observe a “catch up” phenomenon whereby the early benefits of DES in reducing repeat revascularization are attenuated over time. Instead, we found that DES implantation was associated with a significant reduction in the need for future revascularization compared with BMS even at 4 years. Second, we found that the reduction of revascularization was largest among diabetic patients and patients receiving stent length ≥30 mm, where fewer than 10 DES implantations could prevent a TVR event. Finally, despite previous concerns regarding the potential risks of DES in SVGs, no increased risk of myocardial infarction or death was observed at long-term follow-up.
Despite the increased use of arterial grafting, SVGs remain the most commonly used conduit for CABG surgery. Graft atherosclerosis remains a common problem and it is well documented that BMS treatment of SVG lesions is suboptimal because of increased risk of restenosis and graft occlusion (21). Therefore, whether treatment with DES is associated with added benefits in SVG interventions has been a subject of intense debate and the focus of ongoing randomized trials (8). To date, data from 2 small randomized trials comparing DES and BMS for the treatment of SVG lesions have yielded conflicting results (6–8,22). The RRISC trial randomized 38 patients treated with sirolimus-eluting stents and 37 patients treated with BMS. At 30 months, the benefits of DES in reducing repeating TVR were lost and mortality rates were higher with DES (8). In the SOS trial that randomized 39 patients treated with paclitaxel-eluting stents and 41 patients treated with BMS, fewer target revascularizations and no significant increase in myocardial infarction or death was observed in the DES group (8). The ISAR-CABG (Is Drug-Eluting Stenting Associated with Improved Results in Coronary Artery Bypass Grafts) study (23) was recently presented. The investigators randomized 610 patients undergoing SVG interventions to DES versus BMS and found a 50% reduction in target lesion revascularization associated with DES without increased rates of adverse outcomes at 12-months follow-up (23).
Brodie et al. (9) performed 1 of the largest observational studies analyzing SVG interventions among 785 patients receiving DES and 343 patients receiving BMS in the STENT (Strategic Transcatheter Evaluation of New Therapies) registry. At 2 years, the early benefits of DES on repeat TVR were largely attenuated and no longer significantly different compared with BMS. In contrast, we demonstrated that DES use was associated with a sustained reduction of TVR throughout the study period. This discrepancy may be explained by the fact that late repeat revascularization after SVG interventions is often related to disease progression in nonstented areas (24). Therefore, it was believed that the “catch up” phenomenon was due to an imbalance in degenerative SVGs between the treatment groups (9). Although we were unable to quantify the degree of degeneration in SVGs, our study accounted for the age of SVGs in the propensity match, thereby minimizing the difference in disease progression in the nonstented segments between the 2 treatment groups. Our results suggest that DES treatment can provide a significant and sustained benefit in reducing repeat revascularization in SVG interventions.
The large number of patients included in our study afforded an opportunity to perform pre-specified subgroup analyses that provided additional insights. Consistent with the observations regarding DES treatment of native coronary arteries, the association of DES and TVR reduction was largest among diabetics and patients requiring longer stents. By contrast, we did not observe significant difference in TVR among nondiabetic patients treated with DES and BMS in SVG interventions at 4 years. The less robust hazard ratios and the similar TVR rates at 4 years in the nondiabetic subgroup suggest that the benefits of DES may not be as durable as other subgroups.
Another important finding of our paper was the observation that myocardial infarction and mortality rates did not significantly differ in the DES group and the BMS group at a follow-up period of 4 years. In fact, the composite endpoint of myocardial infarction and death was lower in the DES group compared with the BMS group, though it did not achieve statistical significance. Nevertheless, our results are reassuring in demonstrating the safety of DES treatment in SVG interventions in routine clinical practice.
Study limitations
First, our study should be placed in the context of local interventional practice. Ontario has a universal policy whereby all patients over 65 years of age are eligible to receive clopidogrel for 1 year at minimal cost. We have previously demonstrated that more than 70% patients are still compliant with clopidogrel at 6 months (25). Accordingly, the safety profile of DES that was observed in our study may not be generalizable to all healthcare settings. Second, observational studies are subject to the influence of confounding. However, the availability of many clinical variables and a large sample size allowed us to perform a detailed propensity score matched analysis that accounted for all the important potential confounding variables. Finally, we used myocardial infarction after PCI as a safety endpoint because we did not have information on late stent thrombosis in our database. Therefore, although we did not observe significant difference in the rate of myocardial infarction between the treatment groups, we cannot definitely exclude a higher rate of stent thrombosis associated with DES.
Conclusions
DES is associated with significant reduction in the need for repeat revascularization compared with BMS in SVG interventions, and the absolute reduction is largest in patients who are diabetics or have longer lesions. DES use is associated not with an increased risk of myocardial infarction or death compared with BMS. While we await the results of larger randomized clinical trials with long-term follow-up, our results should lend support to the contemporary practice in implanting DES among appropriate patients with SVG lesions.
Appendix
1. : "A polymer-based, paclitaxel-eluting stent in patients with coronary artery disease". N Engl J Med 2004; 350: 221.
2. : "Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery". N Engl J Med 2003; 349: 1315.
3. : "A hierarchical Bayesian meta-analysis of randomised clinical trials of drug-eluting stents". Lancet 2004; 364: 583.
4. : "Drug-eluting stents for saphenous vein graft lesions: the limits of evidence". J Am Coll Cardiol 2009; 53: 929.
5. : "Are our patients better off with drug-eluting stents in saphenous vein grafts?". J Am Coll Cardiol Intv 2009; 2: 1113.
6. : "Randomized double-blind comparison of sirolimus-eluting stent versus bare-metal stent implantation in diseased saphenous vein grafts: six-month angiographic, intravascular ultrasound, and clinical follow-up of the RRISC Trial". J Am Coll Cardiol 2006; 48: 2423.
7. : "Increased late mortality after sirolimus-eluting stents versus bare-metal stents in diseased saphenous vein grafts: results from the randomized DELAYED RRISC Trial". J Am Coll Cardiol 2007; 50: 261.
8. : "Continued benefit from paclitaxel-eluting compared with bare-metal stent implantation in saphenous vein graft lesions during long-term follow-up of the SOS (Stenting of Saphenous Vein Grafts) Trial". J Am Coll Cardiol Intv 2011; 4: 176.
9. : "Outcomes with drug-eluting versus bare-metal stents in saphenous vein graft intervention results from the STENT (Strategic Transcatheter Evaluation of New Therapies) group". J Am Coll Cardiol Intv 2009; 2: 1105.
10. : "Long-term outcomes of drug-eluting stents versus bare-metal stents in saphenous vein graft disease: results from the Prairie “Real World” Stent Registry". Catheter Cardiovasc Interv 2010; 75: 93.
11. : "Comparison of the long-term safety and efficacy of drug-eluting and bare-metal stent implantation in saphenous vein grafts". Circ Cardiovasc Interv 2010; 3: 249.
12. : "Drug-eluting versus bare-metal stent for treatment of saphenous vein grafts: a meta-analysis". PLoS ONE 2010; 5: e11040.
13. : "Drug-eluting or bare metal stents for the treatment of saphenous vein graft disease: a Bayesian meta-analysis". Circ Cardiovasc Interv 2010; 3: 565.
14. : "Drug-eluting stents versus bare-metal stents in saphenous vein graft interventions: a systematic review and meta-analysis". J Am Coll Cardiol Intv 2010; 3: 1262.
15. : "Spurious precision?: Meta-analysis of observational studies". BMJ 1998; 316: 140.
16. : "Late outcomes of drug-eluting versus bare metal stents in saphenous vein grafts: propensity score analysis". Catheter Cardiovasc Interv 2008; 72: 7.
17. : "Safety and Effectiveness of drug-eluting and bare-metal stents for patients with off- and on-label indications". J Am Coll Cardiol 2009; 53: 1773.
18. : "Effectiveness and safety of drug-eluting stents in Ontario". N Engl J Med 2007; 357: 1393.
19. : "A comparison of propensity score methods: a case-study estimating the effectiveness of post-AMI statin use". Stat Med 2006; 25: 2084.
20. : "The use of the propensity score for estimating treatment effects: administrative versus clinical data". Stat Med 2005; 24: 1563.
21. : "Stent placement compared with balloon angioplasty for obstructed coronary bypass grafts". N Engl J Med 1997; 337: 740.
22. : "A randomized controlled trial of a paclitaxel-eluting stent versus a similar bare-metal stent in saphenous vein graft lesions: the SOS (Stenting of Saphenous Vein Grafts) Trial". J Am Coll Cardiol 2009; 53: 919.
23. : "Long-Term Outcomes after Use of Drug-Eluting Stents and Bare Metal Stents for the Treatment of Saphenous Vein Graft Lesions: Results of the Randomized ISAR-CABG Trial: Paper presented at: ACC.11 & i2 Summit; April 4, 2011; New Orleans, LA". http://www.cardiosource.org/acc11coverage. Accessed May 1, 2011.
24. : "Late myocardial ischemic events after saphenous vein graft intervention—importance of initially “nonsignificant” vein graft lesions". Am J Cardiol 1997; 79: 1460.
25. : "Patterns of use of thienopyridine therapy after percutaneous coronary interventions with drug-eluting stents and bare-metal stents". Am Heart J 2009; 158: 592. e1.
Abbreviations and Acronyms
| BMS | bare-metal stent(s) |
| CABG | coronary artery bypass graft |
| CCN | Cardiac Care Network of Ontario |
| DES | drug-eluting stent(s) |
| PCI | percutaneous coronary intervention |
| SVG | saphenous vein graft |
| TVR | target vessel revascularization |
Footnotes
This analysis of the study was funded in part by an operating grant from the
{kind=link}
{kind=link}
{kind=link}
{kind=link}